How to Read a Hospital Bill — Complete Plain English Guide 2026
Hospital bills are designed to be confusing. Not necessarily intentionally — but the complexity of medical billing means that what arrives in your mailbox often looks like it was written in a foreign language.
Codes, acronyms, procedure numbers, revenue codes, adjustment amounts — most patients simply look at the total at the bottom, feel overwhelmed and either ignore the bill or pay it without understanding what they are paying for.
This is exactly how billing errors go undetected. And up to 80% of medical bills contain at least one error.
Understanding your hospital bill is the foundation of everything else covered on FightMedicalBill.com — negotiating, disputing, finding errors and applying for assistance. This plain English guide walks you through every section of a hospital bill so you can read yours with confidence.
The Two Types of Hospital Bills You Will Receive
Most hospital visits generate two completely different types of bills — and many patients do not realise this until they receive the second one.
Type 1 — The Hospital Facility Bill
The facility bill comes from the hospital itself. It covers everything the hospital provided: the room, nursing care, equipment, medications administered during your stay, laboratory services and operating room use.
The facility bill is typically the larger of the two bills and is issued under the hospital’s name.
Type 2 — The Physician Bill (Professional Bill)
Separate from the facility bill, you may also receive one or more bills from individual physicians who provided care during your visit. These typically include:
- Your attending physician or surgeon
- The anaesthesiologist
- Radiologists who read your imaging
- Pathologists who analysed your lab specimens
- Emergency medicine physicians (separate from the ER facility)
- Any consulting specialists
Each of these providers bills separately — which is why a single hospital stay can generate 3, 4, 5 or more different bills from different entities.
This surprises many patients. “I only went to one hospital — why am I getting five bills?” The answer is that while you went to one facility, multiple separate providers delivered your care — each with their own billing entity.
Understanding this distinction is important because:
- Each bill must be checked separately for errors
- Financial assistance applications may need to be filed separately with each provider
- Insurance coverage may apply differently to facility vs physician bills
The Difference Between a Summary Bill and an Itemised Bill
Summary Bill: The document most hospitals send automatically. Shows broad categories of charges — “room and board,” “pharmacy,” “laboratory,” “surgical services” — with totals for each category. This is insufficient for checking errors.
Itemised Bill: The complete line-by-line breakdown of every individual charge. This is what you need to review your bill properly. You have a legal right under HIPAA to request this at any time.
If you have not already requested your itemised bill — do so before reading further. Our guide How to Request an Itemised Medical Bill — Free Script Inside gives you the exact script to use.
Key Information at the Top of Your Bill
Every hospital bill contains identifying information at the top. Here is what each item means:
Patient Name and Date of Birth: Verify these are correct. Wrong patient information can cause insurance claim denials and billing errors.
Account Number: Your unique identifier with this hospital’s billing system. Use this number in all communications with the billing department.
Statement Date: The date the bill was generated — not the date of your visit.
Date of Service (DOS): The date or date range of your hospital visit. Verify this matches your actual admission and discharge dates.
Due Date: The date by which payment is expected. This is a starting point for negotiation — not a final deadline.
Amount Due: The total shown on the summary bill. Do not pay this before reviewing your itemised bill for errors.
Provider Information: The name and address of the billing entity — hospital, physician group or other provider.
Insurance Information: Your insurance carrier name, policy number and group number as recorded by the hospital. Verify these are accurate — errors here cause claim denials.
The Charge Sections on Your Bill
Hospital bills organise charges into categories or departments. Here is what each category typically means:
Room and Board (or Accommodation)
Covers your daily room charge — the cost of your hospital bed, basic nursing care and standard room services. Billed per day based on your room type:
- Medical/surgical room: standard room rate
- Intensive care unit (ICU): significantly higher daily rate
- Step-down or progressive care: intermediate rate
Verify: the number of days matches your actual admission and discharge dates. Room charges for days you were not there — or for an ICU room when you were in a standard room — are common errors.
Pharmacy
All medications administered during your stay — listed by drug name, dose, quantity and unit price. This section is one of the most error-prone areas of hospital billing.
Verify: every medication listed against your memory and any medical records you have. Check that quantities are reasonable for your treatment. Check that brand name medications are not billed when generics were administered.
Laboratory
All laboratory tests — blood tests, urine tests, cultures, biopsies and other specimens. Each test should be listed separately with a CPT code.
Verify: each test was actually ordered for you. Duplicate tests on the same day are a common error. Tests ordered once but billed multiple times are another.
Radiology/Imaging
X-rays, CT scans, MRIs, ultrasounds and other imaging studies. Each study is listed separately.
Verify: each imaging study was actually performed. Compare the list against what you recall or what your discharge papers mention.
Surgical Services
For procedures performed in the operating room. Includes operating room time, surgical supplies and equipment.
Verify: operating room time against your surgical notes if available. Time is typically billed in 15-minute increments — even a 30-minute error at $60+ per minute represents hundreds of dollars.
Anaesthesia
The anaesthesia charge — typically calculated as base units (for the type of procedure) plus time units (for the duration of anaesthesia).
Verify: anaesthesia is typically billed by the minute. Compare the billed time against the operating room start and end times in your surgical notes.
Emergency Department
If you were treated in the emergency room, these charges cover the ER facility fee — separate from the emergency physician’s fee which comes on a separate bill.
Physical/Occupational Therapy
Charges for physical or occupational therapy sessions during your stay.
Verify: the number of sessions matches the actual sessions you received. Therapy charges on your discharge day or days you were not admitted are a common error.
Medical/Surgical Supplies
Individual supplies used during your care — IV supplies, wound care materials, surgical instruments.
Verify: quantities are reasonable for your treatment. Extreme quantities of basic supplies or charges for supplies unlikely to have been used in your specific procedure warrant questions.
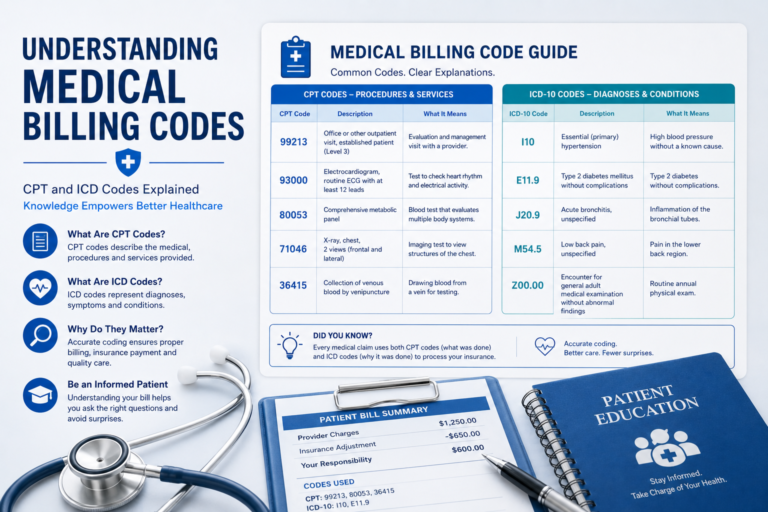
Understanding Medical Billing Codes
Every charge on your itemised bill should have one or more codes attached to it. Understanding what these codes mean helps you verify that charges are correct.
CPT Codes (Current Procedural Terminology)
5-digit codes that describe every medical procedure or service. Assigned by the American Medical Association.
Example: 99283 is an emergency department visit of moderate complexity.
To look up any CPT code: findacode.com (free)
ICD Codes (International Classification of Diseases)
Codes that describe your diagnosis — the reason you needed treatment. ICD-10 codes begin with a letter followed by numbers.
Example: K35.80 is acute appendicitis without abscess.
These codes must be medically consistent with the procedures billed. If an ICD code does not support the CPT procedure billed, the claim may be denied by insurance — or you may have been billed for the wrong procedure.
Revenue Codes
4-digit codes used by hospitals to categorise the department or type of service. Used for insurance billing purposes.
Example: Revenue code 0250 is the pharmacy department.
HCPCS Codes
Alphanumeric codes used primarily for equipment, supplies and drugs. Often used alongside CPT codes.
Example: J0696 is an injection of ceftriaxone (an antibiotic).
NDC Codes (National Drug Codes)
11-digit codes that identify specific medications — including manufacturer, drug and package size. These appear in the pharmacy section of your bill.
Understanding the Financial Columns
Your itemised bill has several financial columns. Here is what each one means:
Billed Charge / Gross Charge
The full, undiscounted price the hospital charges for each service — the “chargemaster rate.” This is always the highest number. Insurance companies and Medicaid pay far less than this amount through their negotiated rates.
Contractual Adjustment / Insurance Discount
The reduction applied because of your insurance company’s negotiated rate with the hospital. This amount is written off — neither you nor your insurance pays it.
Insurance Payment
The amount your insurance company actually paid after applying your deductible and cost-sharing.
Patient Responsibility
The amount you actually owe — after the contractual adjustment and insurance payment have been applied. This is the number that matters most to you.
The difference between the billed charge and your patient responsibility can be enormous — a $30,000 billed charge might result in $2,000 patient responsibility after insurance adjustments.
How to Read Your Explanation of Benefits (EOB)
Your Explanation of Benefits is a document from your insurance company — not the hospital. It shows how your insurance processed the claim. It is not a bill — but it is essential for understanding your bill.
Key sections of your EOB:
Provider Name: The name of the provider who submitted the claim. If this does not match the provider you visited, this may indicate a billing error.
Date of Service: The date the service was provided. Verify this matches your actual visit date.
Service Description: A brief description of what was billed — often a simplified version of the CPT code description.
Amount Billed: The provider’s full charge — the chargemaster rate.
Not Covered Amount: Any amount the insurance company is not covering — either because it is not a covered benefit, or because the claim does not meet coverage requirements.
Discount / Contractual Adjustment: The amount written off because of the insurer’s negotiated rate with the provider.
Plan Paid: The amount your insurance company paid directly to the provider.
Member Responsibility: The amount you owe — your deductible, copay and coinsurance portion.
Reason Codes: Short codes explaining any adjustments or denials. Always look these up — they tell you exactly why a charge was reduced or denied.
Comparing Your EOB to Your Hospital Bill
One of the most powerful error-detection steps is comparing your hospital bill to your EOB. Discrepancies between the two are major red flags:
The hospital billed for services not on your EOB: Services billed directly to you that were never submitted to insurance — possible billing error or balance billing violation.
The hospital billed amounts different from your EOB: Your patient responsibility on the hospital bill does not match your member responsibility on the EOB — possible billing error.
The EOB shows a denial you were not notified about: Your insurance denied part of the claim — you need to investigate why and whether to appeal.
Confusing Items That Appear on Hospital Bills
Several items commonly appear on hospital bills that confuse patients. Here is what they actually mean:
Facility Fee
An additional charge for using a hospital facility — separate from the physician’s fee. Facility fees apply when you receive care at a hospital-based clinic, even for outpatient services. These are legitimate charges but patients are often not warned about them in advance.
Observation Status vs Inpatient Admission
Your billing status during a hospital stay — inpatient or outpatient observation — significantly affects what you pay. Patients kept in observation status are technically outpatients, which means different cost-sharing applies under Medicare and many private insurance plans.
If you stayed overnight but your bill says you were in observation, ask the hospital whether your status can be reviewed. The decision of whether to admit you as inpatient or keep you in observation has major billing implications.
Chargemaster Rate
The hospital’s internal list price for every service — always much higher than what insurance actually pays. Uninsured patients are sometimes initially billed at chargemaster rates. Always ask for a self-pay discount or apply for charity care rather than paying chargemaster rates.
Cost Report
Some bills include a reference to the hospital’s cost report — a federal filing that shows actual costs versus charges. This is technical information used in Medicare billing analysis.
Modifier Codes
Two-digit codes added to CPT codes to provide additional information about how a service was performed. Modifier -50 means a bilateral procedure. Modifier -25 means a significant evaluation on the same day as a procedure. Modifiers affect reimbursement amounts — incorrect modifiers can cause over- or under-billing.
The Hospital Bill Error Checklist — Use Before Paying
Work through this checklist on every hospital bill over $500 before making any payment:
Patient Information
[ ] Is your name spelled correctly?
[ ] Is your date of birth correct?
[ ] Is your insurance information accurate?
[ ] Are the admission and discharge dates correct?
Charges Review
[ ] Have I requested the complete itemised bill?
[ ] Are there any duplicate line items?
[ ] Are there any charges for services I do not remember receiving?
[ ] Do the room charges match my actual days in hospital?
[ ] Are laboratory tests listed that were not ordered?
[ ] Are medication quantities reasonable?
[ ] Are brand name medications listed when I received generics?
[ ] Do the operating room minutes match my surgical records?
[ ] Are there physical therapy charges on days I was not treated?
Codes Review
[ ] Have I looked up any CPT codes I do not recognise?
[ ] Do the ICD diagnosis codes match my actual condition?
Financial Review
[ ] Have I compared this bill to my EOB?
[ ] Does my patient responsibility on the bill match my member responsibility on the EOB?
[ ] Have I checked for balance billing on in-network services?
[ ] Have I researched fair market prices for major procedures?
A Real Hospital Bill — Walk-Through Example
Let us walk through a simplified example of what a hospital bill looks like and how to read each section.
Patient: Jane D.
Date of Service: March 15, 2026
Facility: Metro General Hospital
Reason for Visit: Emergency appendectomy
Summary Bill Received:
Emergency Department Services: $4,200
Laboratory: $1,850
Radiology/CT Scan: $3,100
Surgical Services: $18,400
Operating Room — Anaesthesia: $6,800
Pharmacy: $2,300
Room and Board (1 day post-op): $2,800
Medical/Surgical Supplies: $1,400
Total Billed: $40,850
Insurance Contractual Adjustment: -$24,510
Insurance Payment: -$10,848
Patient Responsibility: $5,492
What Jane should do next:
Step 1 — Request the itemised bill
The summary shows broad categories. Jane needs the line-by-line breakdown to check each charge.
Step 2 — Review the laboratory charges
$1,850 for laboratory work on an appendectomy case. Jane should check what tests were run and confirm each one is on her itemised bill only once.
Step 3 — Verify operating room time for the anaesthesia charge
$6,800 for anaesthesia — Jane should compare the billed time against the surgical notes showing when surgery began and ended.
Step 4 — Check pharmaceutical charges
$2,300 for pharmacy — Jane should review each medication listed, verify quantities and confirm no brand-name medications were charged when generics were given.
Step 5 — Compare to EOB
Jane’s EOB from her insurance company should show similar amounts. Any discrepancy between her EOB and the hospital bill warrants investigation.
Step 6 — Look up CPT codes
If any charge description is unclear, Jane looks up the CPT code at findacode.com to understand exactly what was billed.
What Jane found:
- One duplicate laboratory charge for a complete blood count ($185 charged twice)
- Anaesthesia billed for 2 hours 45 minutes — surgical notes showed 2 hours — overcharge of approximately $400
- One medication listed that does not appear in her nursing notes
Total potential overcharges identified: $785+
This is a typical result for a patient who takes the time to review their bill systematically.
Tools and Resources for Reading Your Bill
Free CPT Code Lookup:
- findacode.com — search any 5-digit CPT code
- aapc.com/codes — comprehensive code search
Fair Market Price Research:
- healthcarebluebook.com — fair prices by procedure and zip code
- fairhealthconsumer.org — typical costs by CPT code
Hospital Price Transparency:
- cms.gov/hospital-price-transparency — hospital standard charges
Medical Records Request:
- Request from the hospital’s Health Information Management department
- You have a HIPAA right to your records within 30 days of request
- Some hospitals have patient portals where records are available online
What to Do After Reading Your Bill
Once you have read and reviewed your hospital bill, here is what comes next depending on what you find:
If you found billing errors:
See our guide: Medical Billing Errors — How to Find and Fix Them — for the exact steps and scripts to dispute each error.
If you cannot afford to pay what you owe:
See our guides:
- What to Do If You Can’t Pay a Hospital Bill — 6 Options
- Hospital Financial Assistance Programs — The Complete Guide
- Medical Debt Forgiveness Programs 2026 — The Complete List
If your insurance denied part of the claim:
See our guide: How to Dispute a Medical Bill With Your Insurance Company
If you received a surprise out-of-network bill:
See our guide: Surprise Medical Bills — Your Rights Under the No Surprises Act
If you want to negotiate the balance down:
See our guide: How to Negotiate Medical Bills After Surgery — Save Up to 80%
Frequently Asked Questions
Why is the amount billed so much higher than what insurance actually pays?
Hospitals set their chargemaster rates — their full list prices — at artificially high levels. Insurance companies then negotiate rates far below these list prices as a condition of being included in the hospital’s network. The difference is written off as a contractual adjustment. Uninsured patients who do not know to ask may be initially billed at chargemaster rates — always ask for the self-pay discount or apply for charity care.
Why did I receive multiple bills from one hospital visit?
Each independent provider who treated you during your visit bills separately — the hospital facility, the emergency physician group, the anaesthesiologist, the radiologist, the pathologist and any consulting specialists all bill independently. This is standard practice in US healthcare and can result in 4 to 6 separate bills from a single visit.
What does adjustment mean on my hospital bill?
An adjustment is a reduction in the billed charge. The most common adjustments are contractual adjustments — reductions to the negotiated rate agreed between the hospital and your insurance company. Adjustments can also reflect corrections, billing errors or discounts applied.
What is a Revenue Code and do I need to worry about it?
Revenue codes are 4-digit numbers hospitals use to categorise services for insurance billing. They appear on the UB-04 claim form used for hospital billing. You do not need to understand revenue codes for basic bill review — but if a charge does not have a revenue code or has an unusual one, it may warrant investigation.
My bill shows a balance after insurance paid — is this always correct?
Not always. Compare your bill to your EOB carefully. Common discrepancies include: the hospital applying your deductible to services that your insurance records as already met, billing errors that affect how insurance processes the claim, and balance billing for in-network services which may violate your insurance contract or the No Surprises Act.
How long do I have to pay my hospital bill?
Most hospitals expect payment within 30 days but typically do not send accounts to collections until 90 to 180 days after the bill is generated. You have more time than the due date suggests — and engaging with the hospital to negotiate, apply for assistance or set up a payment plan prevents collections activity regardless of whether you meet the original due date.
Can the hospital share my medical billing information with credit bureaus without my consent?
Hospitals can report unpaid debts to credit bureaus — but under the 2023 changes, unpaid medical debt cannot be reported for the first 12 months, medical debt under $500 is not reported and paid medical debt is removed immediately. Hospitals typically cannot share the medical details of what care you received — only the financial information about unpaid balances.
Your Hospital Bill Reading Action Plan
When you receive any hospital bill:
- Note the account number, date of service and total amount due
- Request the complete itemised bill — do not review only the summary
- Request your EOB from your insurance company if you have insurance
- Work through the error checklist in Part 3 of this guide
- Look up any CPT codes you do not recognise at findacode.com
- Compare your bill to your EOB — note any discrepancies
- Research fair market prices for major procedures at healthcarebluebook.com
- Make a list of every charge that is unclear, suspicious or potentially incorrect
- Call the billing department with your specific list of questions
After reviewing:
- Dispute any errors — use our guide: Medical Billing Errors — How to Find and Fix Them
- Check financial assistance eligibility — use our guide: Hospital Financial Assistance Programs
- Negotiate any legitimate remaining balance — use our guide: How to Negotiate Medical Bills After Surgery
Reading your hospital bill is the first and most important step in taking control of your medical costs. Understanding what you are being charged — and why — puts you in a position to identify errors, negotiate effectively and access every option available to reduce what you owe.
Medical and Financial Disclaimer: The information on FightMedicalBill.com is for educational purposes only and does not constitute medical, legal or financial advice. Medical billing practices, code definitions and insurance processing rules change regularly. Always verify information with your specific provider and insurance company.